
Health Canada Approved Clorotekal (Chloroprocain HCl, Inj USP 1%)
Indications
CLOROTEKAL (chloroprocaine hydrochloride injection) is indicated for:
- the induction of spinal anaesthesia by intrathecal administration, in adults undergoing surgical procedures no longer than 40 minutes in duration.
Contraindications
CLOROTEKAL is contraindicated:
- in patients who are hypersensitive to this drug, medicinal products of the PABA (para-ami-nobenzoic acid) ester group, or to any ingredient in the formulation, including any non-me-dicinal ingredient, or component of the container. For a complete listing, see 6 DOSAGE FORMS, STRENGTHS, COMPOSITION AND PACKAGING.
- in patients with general and specific contraindications to spinal anaesthesia regardless of the local anaesthetic used, should be taken into account (e.g. decompensated cardiac in-sufficiency, hypovolemic shock).
- for intravenous regional anaesthesia (IVRA).
- in patients with serious problems with cardiac conduction.
- in patients with severe anaemia.
- in patients taking anticoagulants or those with congenital or acquired bleeding disorder.
- in patients with septicemia or local infection at the site of the proposed lumbar puncture.
*Clorotekal is a registered trademark of Sintetica S.A. Imported and distributed by B. Braun of Canada Ltd.
Key Information
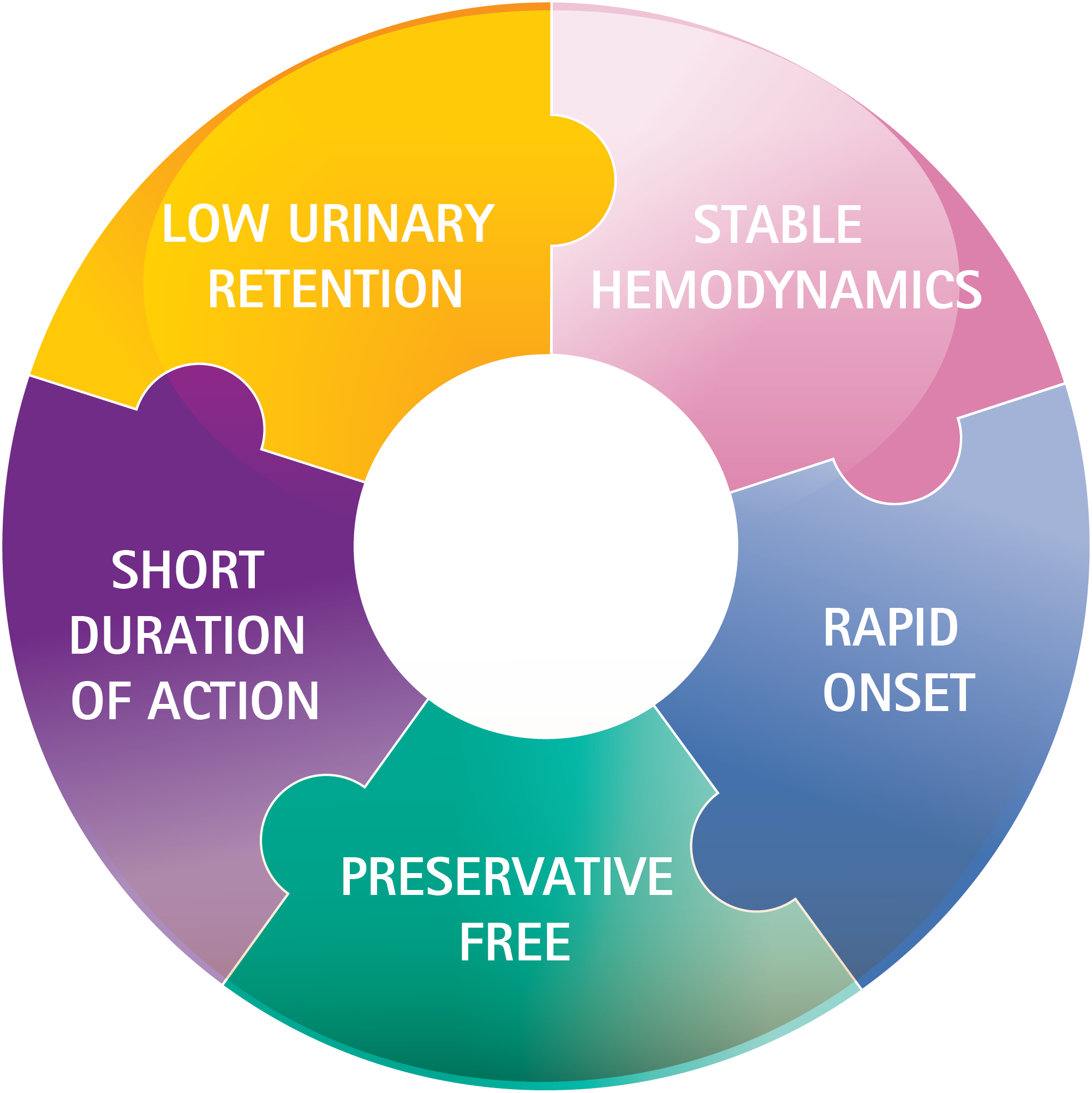
One Solution - Many Benefits
ULTRA SHORT DURATION OF ACTION
PRESERVATIVE-FREE: Clorotekal is formulated without sodium bisulfate or methylparaben.
RAPID ONSET: Clorotekal has a rapid onset of action, usually 6 to 12 minutes.
LOW URINARY RETENTION
STABLE HEMODYNAMICS
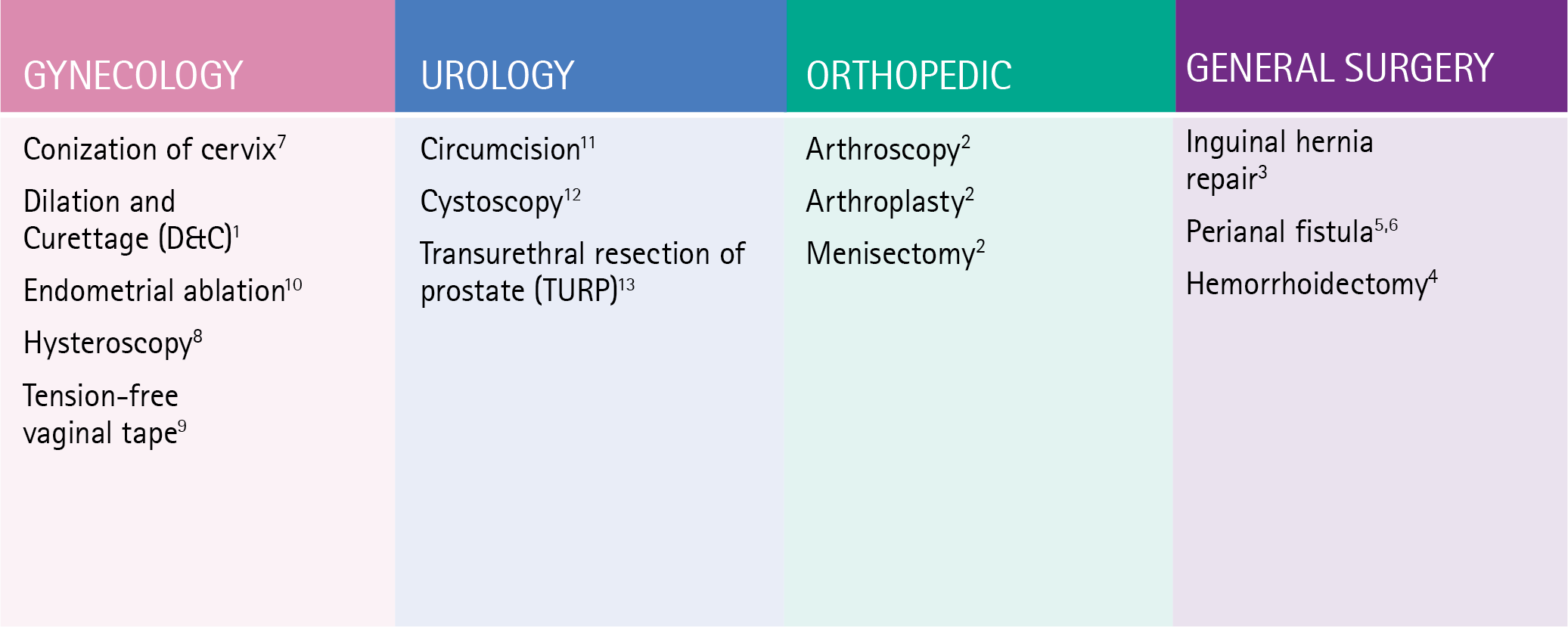
EXAMPLES OF SURGICAL PROCEDURES THAT MAY BE SUITABLE FOR CLOROTEKAL’S SHORT DURATION OF ACTION
Clinical Studies of 1% Chloroprocaine
STUDY 1* – Efficacy and Tolerability
Study Design:
- Study 1 was a phase 2 single-center, prospective, randomized, observer-blinded study.
- Evaluated the efficacy and the tolerability of 1% chloroprocaine in three doses 30, 40, and 50 mg after spinal injection.
- In 45 adult patients undergoing short duration (<40 minutes) lower limb surgery.
Efficacy Results:
- Neither rescue anesthesia nor rescue analgesia was required for subjects randomized to chloroprocaine 50 mg.
- Three subjects in the 30 mg dose group and three subjects in the 40 mg dose group required intraoperative rescue medications.
- Doses above 50 mg have not been adequately tested for efficacy and safety.
*Spinal anesthesia with Chloroprocaine HCl 1% for elective lower limb procedures of short duration: a prospective, randomized, observer-blinded study in adult patients.
STUDY 2* – Chloroprocaine Compared to Bupivacaine
Study Design:
- Study 2 was a phase 3, multicenter, prospective, randomized, observer-blinded study.
- Evaluated the safety and efficacy of 50 mg of chloroprocaine 10 mg/mL in intrathecal anesthesia versus 10 mg of bupivacaine 0.5%.
- In 130 adult patients undergoing short duration (<40 minutes) low abdominal surgery (gynecological or urological) and lower limb surgery.
- Each patient received a single dose of anesthetic: 50 mg of chloroprocaine or 10 mg of bupivacaine.
Efficacy Results:
- Efficacy was determined by the proportion of patients who were able to complete the surgical procedure without the need for rescue intravenous analgesic or sedation drugs.
- Efficacy results proved that 6 of 66 subjects (9%) in the chloroprocaine group required rescue compared to 6 of 64 (9%) in the bupivacaine group.
*Prospective, observer-blinded, randomized clinical study to investigate and compare the efficacy of intrathecal plain solutions containing Chloroprocaine 1% (50 mg) versus Bupivacaine 0.5% (10mg)
Product Details
Product Size:
50mg/5mL
Product Code (10 mg/mL)
D7055-00